
Strep A
in children
Know Your Enemy: A spotlight on Strep A in children
By Dr Emma Goeman
Published December 2023
The rising threat of Strep A in children
Streptococcus pyogenes, also known as Group A streptococcus or Strep A, is an increasingly common cause of life-threatening disease, termed invasive group A streptococcal infection (iGAS), especially in children. A spike in iGAS cases in Australia, including some with devastating outcomes, has received media coverage in the past 9-12 months.1,2,3,4 iGAS is now a notifiable condition in all Australian states and territories, and jurisdictions commenced reporting at different times throughout 2021 and 2022. Even taking into account changes to reporting, recent high incidence rates in Australia are causing considerable concern.
Recent trends in iGAS infections
Pre-pandemic, rises in iGAS occurred in several high-income countries. However, rates dropped substantially in 2020-2021, likely due to measures implemented to reduce the spread of COVID-19. Data from the Paediatric Active Enhanced Disease Surveillance (PAEDS) Network showed that in Australian children aged 0 – 17 years, iGAS rates in 2022 sharply rose to 5.2 per 100,000 children in the third quarter and remained unseasonably high in the fourth quarter. Aboriginal and Torres Strait Islander children experienced incidence rates 1.8 times higher than non-Indigenous children during 2018 - 2022. Pneumonia and bacteraemia were the most common clinical syndromes. 32% of cases were severe and there were 3 deaths (1%).5 Mortality rates are substantially higher in adults, particularly in the presence of necrotizing fasciitis, also known as “flesh-eating disease”. Data from the National Communicable Diseases Surveillance Dashboard shows that high iGAS case numbers are showing no signs of slowing down in 2023.6
Diverse clinical manifestations of Strep A infections
Strep A may live harmlessly in the throat and is transmitted via respiratory droplets and direct contact with infected skin sores. Common clinical syndromes include tonsillitis and impetigo (see Figure 1), which are generally mild, as well as scarlet fever. More severe disease manifestations include sepsis, meningitis, pneumonia, bone, joint, and deep tissue infections, toxic shock syndrome, and necrotizing fasciitis.

Figure 1 – Image shows an impetigo skin infection, also known as school sores.
Strep A is also the cause of acute post-streptococcal glomerulonephritis and acute rheumatic heart disease, which can lead to chronic kidney damage and rheumatic heart disease. Aboriginal and Torres Strait Islander Australians have long borne the brunt of some of the highest rates in the world.
Recognising sepsis
Where minor Strep A infections may progress into an emergency can be challenging to discern clinically. Therefore, it always helps to consider, “Could this be sepsis?”15
Sepsis is defined as a life-threatening condition that develops when the body’s response to an infection injures its own tissues and organs. When shock ensues, it can be rapidly fatal.7Signs of sepsis in young children may include:8
- An altered conscious state (characterised by lethargy, irritability, floppiness, or a weak cry).
- An unwell appearance or high level of parental concern.
- A rash (which in the case of Strep A often resembles sunburn and may feel like sandpaper).
- Features of impaired circulation, such as reduced peripheral perfusion, pale, cool, or mottled skin, tachycardia, or decreased urine output.
- Tachypnea or grunting.
- Unexplained pain.
- Fever or hypothermia.
Toxin-mediated disease may be heralded by fever, vomiting, diarrhoea (which can be mistaken for gastroenteritis), myalgia, conjunctival injection, confusion, collapse, and a widespread erythematous rash.8
If sepsis is suspected, blood cultures should ideally be collected prior to the commencement of antibiotics as part of a bundle of care with initial resuscitation. However, collection should not cause a delay in antibiotic administration.9
Optimising blood culture collection
The most important factor in optimising the diagnostic yield of a blood culture is the volume of blood; more blood equals better sensitivity.
- The minimum acceptable volume of blood in a paediatric blood culture bottle is 0.5 mL, but ideally, at least 1 mL should be collected, even from newborns.
- For most preschool-aged children over the age of 12 months, the target volume is 4 mL.
- Adult aerobic and anaerobic blood culture bottles can be used for school-aged children and adolescents, with volumes of 5 - 10 mL per bottle.
- For adults, a recommended total collection is 40 –60 mL (2 - 3 sets of aerobic and anaerobic bottles, approximately 4 - 6 bottles, each containing 10 mL of blood inoculated) for adequate sensitivity.
Blood culture bottles should not be overfilled. Collection should be performed using strict aseptic technique via peripheral venipuncture to minimise the risk of contamination.
Laboratory detection of Strep A
Strep A is easily cultured and recognised in the laboratory on routine clinical samples. Throat swabs will pick up Strep A, causing pharyngitis and tonsillitis, as well as asymptomatic colonisation. Skin swabs from sores and open wounds will detect Strep A, causing impetigo, abscesses, and cellulitis. Culture of body fluids and tissues will aid in the diagnosis of invasive, deeper infections. Growth of Strep A in a child’s urine usually reflects localised skin infection around the genital area, especially vulvovaginitis in pre-pubertal females, but may rarely reflect bloodstream infection with spillover into the urine.
Blood cultures are continuously monitored by an automated instrument in the laboratory for 5 days. The vast majority of significant pathogens will be detected within the first 48 hours of incubation. Treating clinicians will be notified of a positive blood culture result immediately. Initially, only the Gram stain characteristics of the organism will be known, such as Gram-positive cocci (see Figure 2) resembling streptococci. Further organism identification and susceptibility testing requires growth on solid media (agar plates) and takes a further 24- 48 hours.
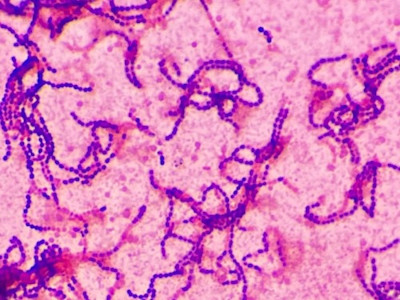
Figure 2 – Image shows Gram-positive cocci in chains.
Antibody tests (anti-streptolysin O titre, or ASOT, and anti-DNase B antibodies) are used to detect recent past Strep A infection, to aid in the diagnosis of complications such as acute post streptococcal glomerulonephritis and acute rheumatic fever. It is preferred to collect two samples 2-4 weeks apart to detect rising antibody levels. Strep A can also complicate viral infections such as varicella, influenza, and COVID-19, as well as other respiratory viruses for which PCR tests are available.
Antibiotic resistance and treatment options
Strep A is universally susceptible to penicillin, and therefore, to amoxicillin, ampicillin, cephalexin, and flucloxacillin. Penicillins are the mainstay of treatment. However, resistance to other agents is increasing, with resistance rates to erythromycin, clindamycin, and tetracycline reaching 8.7%, 7.1%, and 18.7%, respectively, in Australia-wide data from 2019.10
Cotrimoxazole is a useful alternative agent in certain settings, such as in patients with immediate severe or delayed severe penicillin allergy and clindamycin resistance. This is also the case when there is co-infection with Staphylococcus aureus, particularly MRSA. In remote settings, cotrimoxazole is preferred due to its low cost, twice-daily dosing, and good tolerability, especially in children.11,12
In a hospital setting, clindamycin is often added to benzylpenicillin for its anti-toxin effects, and intravenous immunoglobulin is given as an adjunctive treatment in severely septic individuals.
Preventative strategies and the search for vaccines
At a population level, preventative strategies for strep A infections include improving the social determinants of health, which involves improving skin health, including controlling scabies infections, particularly in remote communities in Northern Australia. Additionally, the race is on to find the best vaccine among a selection of candidate vaccines.13 The promotion of respiratory and hand hygiene practices may also interrupt transmission.
On a more individual and community level, some jurisdictions recommend preventative antibiotics for household contacts of individuals with iGAS, similar to the model of care for meningococcal disease. This is because the risk of secondary cases of iGAS in this group is 2,000 times higher than that in the general population in the 30 days following exposure.14
If you enjoyed this article, subscribe to our electronic Pathology Focus newsletter.
References
- https://www.theguardian.com/australia-news/2023/aug/23/cases-of-flesh-eatinginvasive-strep-a-bacteria-surge-in-australian-children#:~:text=The paper included nationally invasive,was 1%2C185%2C the paper said.
- https://www.mcri.edu.au/news-stories/australia-experiences-intense-surge-in-strep-acases-similar-to-northern-hemisphere-wave
- https://www.medicalrepublic.com.au/child-dies-as-strep-a-spreads/87141
- https://www.theage.com.au/national/victoria/two-children-die-amid-marked-increasein-invasive-strep-a-infections-20230103-p5ca0e.html
- Abo, Yara-Natalie et al. Increase in invasive group A streptococcal disease among Australian children coinciding with northern hemisphere surges. The Lancet Regional Health – Western Pacific, Volume 0, Issue 0, 100873
- Hla TK, Cannon JW, Bowen AC, Wyber R. Getting to grips with invasive group A streptococcal infection surveillance in Australia: are we experiencing an epidemic? Medical Journal of Australia 2023, volume 219, issue 6, pp. 242-245
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):801-10. doi:10.1001/jama.2016.0287. PMID: 26903338; PMCID:PMC4968574.
- The Royal Children’s Hospital, Melbourne, Australia, Clinical Practice Guideline on Sepsis – Assessment and Management [Internet, last updated March 2020; cited 8/10/2023], Available from: https://www.rch.org.au/clinicalguide/guideline_index/SEPSIS_assessment_and_management/
- Weiss, S.L., Peters, M.J., Alhazzani, W. et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Intensive Care Med 46 (Suppl 1), 10–67 (2020). https://doi.org/10.1007/s00134-019-05878-6
- Australian Commission on Safety and Quality in Health Care. AURA 2021: fourth Australian report on antimicrobial use and resistance in human health. Sydney: ACSQHC; 2021.
- Bowen AC, Lilliebridge RA, Tong SY, Baird RW, Ward P, McDonald MI, Currie BJ, Carapetis JR. Is Streptococcus pyogenes resistant or susceptible to trimethoprimsulfamethoxazole? J Clin Microbiol. 2012 Dec;50(12):4067-72. doi: 10.1128/JCM.02195-12. Epub 2012 Oct 10. PMID: 23052313; PMCID: PMC3502963.
- Bowen AC, Carapetis JR, Currie BJ, Fowler V Jr, Chambers HF, Tong SYC. Sulfamethoxazole-Trimethoprim (Cotrimoxazole) for Skin and Soft Tissue Infections Including Impetigo, Cellulitis, and Abscess. Open Forum Infect Dis. 2017 Nov 2;4(4):ofx232. doi: 10.1093/ofid/ofx232. PMID: 29255730; PMCID: PMC5730933.
- Walkinshaw, D.R., Wright, M.E.E., Mullin, A.E. et al. The Streptococcus pyogenes vaccine landscape. npj Vaccines 8, 16 (2023). https://doi.org/10.1038/s41541-023-00609-x
- Carapetis JR, Jacoby P, Carville K, Ang SJ, Curtis N, Andrews R. Effectiveness of clindamycin and intravenous immunoglobulin, and risk of disease in contacts, in invasive group a streptococcal infections. Clin Infect Dis. 2014 Aug 1;59(3):358-65. doi:10.1093/cid/ciu304. Epub 2014 Apr 29. PMID: 24785239.
- Australian Commission on Safety and Quality in Healthcare (ACSQHC) Quality Statement 1 - Could it be sepsis? https://www.safetyandquality.gov.au/standards/clinical-care-standards/sepsis-clinical-care-standard/quality-statements/qualitystatement-1-could-it-be-sepsis Accessed 15/11/23.
Figure 1. Reproduced with permission from ©DermNet www.dermnetnz.org 2023.
About the Author

Dr Emma Goeman
MBBS(Hons) BA MPHTM FRACP FRCPADr Emma Goeman
MBBS(Hons) BA MPHTM FRACP FRCPA- perinatal and paediatric infections
- antimicrobial resistance
- antimicrobial stewardship
- vaccine preventable diseases
- forensic microbiology
After graduating from the University of Melbourne in 2005, Dr Emma Goeman trained in paediatrics, infectious diseases and clinical microbiology in Melbourne, Alice Springs and Sydney. She obtained Fellowships of the RACP (Infectious Diseases, Paediatrics and Child Health Division) and RCPA (Microbiology) in 2017. Having joined the team at Australian Clinical Labs as a Clinical Microbiologist in October 2022, Dr Goeman also works as a Staff Specialist in Immunisation for the National Centre for Immunisation Research and Surveillance (NCIRS), and has an appointment as a Clinical Senior Lecturer for the University of Sydney. Previously Dr Goeman also worked as an Infectious Diseases Physician and Clinical Microbiologist at a large public tertiary hospital in Sydney.
Local Pathologists
 Pathologist
Pathologist
 Pathologist
Pathologist
Related Pages

Assessing Allergy in Clinical Practice
Associate Professor Louise Smyth explains the clinical significance of allergy, immune responses and the role of accurate testing in managing allergic conditions.

Calprotectin & IBD
Associate Professor Louise Smyth discusses the role of calprotectin testing in the diagnosis and management of IBD.

Managing Vitamin D Deficiency
Dr Phoebe Stanford highlights the role of vitamin D, health risks of deficiency, and guidance on MBS testing and result interpretation.